|
 |
|
Mihama Nuclear Power Plant across the bay.
|
|
|
As most people will be aware from reports in the mainstream media, on August 9th, the 59th anniversary of the bombing of Nagasaki, there was a serious accident at the Mihama-3 reactor, located in Fukui Prefecture. Serious? Yes, in the commonly understood sense of the word, though it was only awarded a 0+ rating on the International Nuclear Event Scale (i.e. between 'no safety significance' and 'anomaly'). No doubt it would have been swept under the carpet as just another minor steam leak if it weren't for the inconvenient fact that eleven people were hospitalized, five of whom died.
So how serious was it and why was it given a rating of only 0+ on the INES scale? These and other questions will be addressed below, but first a brief run-down of what actually happened.
What actually happened?
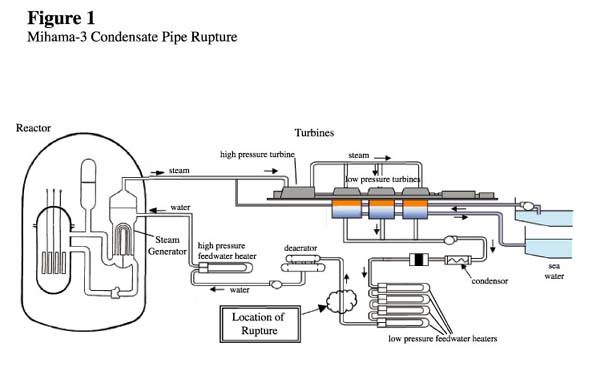
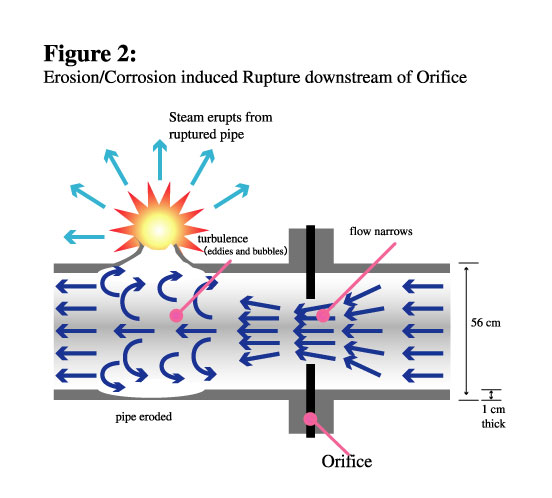
At 15:22 a fire alarm went off in the turbine building of Kansai Electric Power Company's (KEPCO) Mihama-3 reactor (PWR, 826 MW). A main condensate pipe in the secondary coolant system1 had ruptured (see figure 1). The pipe2 contained water heated to 140 degrees Celsius under 9.5 atmospheres pressure. When the pipe ruptured, this water spewed out in the form of steam, severely scalding the unfortunate workers who happened to be in the room. The thickness of the wall of the pipe at the point where it ruptured was down to around 1mm, compared to the original thickness of 10mm and the regulatory minimum of 4.7mm. It had never been checked during the entire 28 years that the plant had been operating.
The sequence of events from there on can be summarized as follows:
|
Time
|
Action
|
| August 9th |
|
|
15:26
|
Operators begin to manually turn off of the generator
|
|
15:28
|
Reactor trip due to shortage of feedwater to loop A steam generator3
|
|
15:28
|
Auxiliary feedwater pumps activated (both turbine-powered and electric motor-powered pumps)
|
|
15:35
|
Hot shutdown stability confirmed
|
|
15:44
|
Dearator valve closed (upstream of ruptured pipe)
|
|
15:58
|
Injection of boric acid4 into reactor coolant system
|
|
16:05
|
Main steam isolation valve closed (downstream of generator)
|
|
16:26
|
Feedwater isolation valve closed (upstream of generator, downstream of ruptured pipe). The leakage of steam and water continued until this moment.
|
|
16:55
|
Water level in steam generator at 33%
|
|
17:12
|
Turbine-powered auxiliary feedwater pump stopped. (Electric pump continues to operate.) Its outlet flow control valves (A, B, and C) were shut manually.
|
|
17:13
|
Operators tried to reopen these control valves to 60%, but valves A and C did not respond.
|
| August 10th |
|
|
19:05
|
Cold shutdown achieved
|
KEPCO's estimate is that a total of 800 tons of water escaped. The basis for this estimate is not yet clear, but apparently around half of this was from the secondary coolant system and half from the auxiliary feedwater system. There had been 1,100 tons in the secondary coolant system to start with.
Who was in the building?
At the time of the accident the plant was operating at full power. One hundred and five workers were in the turbine building making preparations for a periodic inspection that was to begin on August 14th. By carrying out preparatory work while the plant was still operating, KEPCO hoped to minimize downtime and reduce costs. The building itself has three floors, so not all of the people in the building came into direct contact with the steam. Also, over a hundred other workers, who had been in the building shortly before the accident, were taking a break outside. The eleven people who were hospitalized were all employees of Kiuchi Instruments, a subcontractor whose job was to maintain measuring instruments, such as pressure gauges and thermometers. Four of the injured workers were dead on arrival and a fifth died on August 25th.
How serious?
Let us now return to the question of how serious the accident was and why it was only classified as a 0+ accident5. To deal with the latter question first, KEPCO claimed that monitors recorded no radiation. This appears to have been the principal criterion considered. We have no grounds to challenge KEPCO's claim regarding the recording on its radiation monitors, but we would assume that a small amount of radioactivity would have been released, even if the monitors didn't detect it. In particular, we would expect some tritium to have escaped with the steam and water, although the quantity may well have been very low. The reason for a minimal release of radioactivity is that the secondary coolant system of Pressurized Water Reactors (the type used at all KEPCO nuclear power plants) does not pass directly through the reactor itself. Instead, heat from the reactor is carried by the primary coolant system to the steam generator, which acts as a heat exchanger. There the heat is transferred to the coolant in the secondary system. This is then forced through the turbines in the form of steam. This is the principal difference between Pressurized Water Reactors (PWR) and Boiling Water Reactors (BWR). In the latter case, water flows through the reactor, where it is converted to steam, which is sent directly to the turbines. Consequently, the radioactivity of the steam passing through the turbines in BWRs is much greater than in PWRs.
However, despite the fact that little radioactivity escaped, this was indeed a serious accident. The loss of life is only one of several reasons for passing this judgment. Other reasons include the dangers inherent in the loss of coolant, even if it was 'only' secondary coolant, and the dangers associated with the woefully inadequate nuclear safety system in Japan, revealed once again through this accident.
Loss of coolant
The problem with a loss of coolant accident (LOCA) is that it could lead to a reactor meltdown, as occurred in the 1979 Three Mile Island (TMI) accident. The most serious case is where there is a loss of primary coolant, since it is this which directly cools the reactor. However, if there is nowhere for the heat from the primary coolant system to go, the heat in the reactor will continue to build up. The secondary coolant is there to remove this heat and channel it off to produce electricity. That is the theory behind the fear of a LOCA. The comparison with TMI is instructive, because like Mihama-3 it was a PWR and like Mihama-3, the problem started with a fault in the secondary coolant system. In the TMI case, a valve failure in the condensor prevented the secondary coolant from circulating. Hence, it was no longer able to remove heat from the primary coolant. This was compounded by a series of other failures, which led to a loss of primary coolant and core meltdown. In the Mihama case back-up systems worked (more or less) and the primary system, including the reactor core, did not overheat. Ironically, after the situation had been stabilized, the auxiliary feedwater pump was turned off and then its outlet valves were tested once again (see time-line above). On this occasion two of them failed. One hates to think what might have happened if they had failed when they were needed in the first place. Catastrophes occur when failures in one component of the system are compounded by failures in other components. But the word 'catastrophe' doesn't appear on the INES scale (not a word the nuclear industry likes to use). The highest classification, level 7, of which Chernobyl is an example, is 'Major Accident'. However, if we choose to employ labels in accordance with their commonly understood meanings, then I think everyone will agree that Chernobyl was a catastrophe and Mihama-3 was a serious accident.
In the Mihama-3 case, perhaps even more serious than the accident itself was the proof that it provided that the nuclear safety system in Japan is woefully ineffective. To understand this we need to take a look in some detail at the history behind the accident.
History
Mihama-3 is an old reactor. When it commenced operations, back in 1976, little was known about erosion and corrosion of the piping in nuclear power plants. The feedwater pipes in the secondary coolant system were expected to see out the life of the reactors (nominally 40 years). However, a very similar accident to the Mihama-3 accident, which occurred in 1986 at the Surry-2 reactor, and the discovery in 1987 of serious thinning of pipes in the Trojan reactor (both in the USA) showed that this complacency was unjustified. The response of the Japanese nuclear industry and regulators, citing various differences between the situation in Japan and the US, was to say that it couldn't happen here. Nevertheless, the industry developed guidelines for checking pipes in the secondary coolant system.
These guidelines came into operation in 1990, although their implementation is voluntary, reflecting the low priority accorded to the secondary coolant system. The guidelines recommend various locations that should be checked. Of particular relevance to this case, they include locations within a distance of twice the pipe diameter from potential sources of turbulence. One such source is a so-called 'orifice' flowmeter (figure 2). The Mihama-3 pipe ruptured at almost exactly 2 diameters downstream from one of these. The orifice narrows the space through which the water flows and the pressure difference upstream and downstream of the orifice is used to measure the flow. However, it is recognized that the turbulent flow caused by the orifice increases the rate of pipe erosion, so the thickness of the pipe should be checked more regularly than other areas.
All PWRs in Japan were manufactured by Mitsubishi Heavy Industries (in partnership with Westinghouse). At the time the above guidelines were drafted Mitsubishi was also the prime maintenance contractor. Mitsubishi compiled a list of locations that it thought should be inspected, but for some reason the location where the pipe ruptured at Mihama-3 was not included on the list. Investigations since the accident have revealed that this same location was left off the list at four other reactors, including reactors owned by KEPCO, but also including reactors belonging to other power companies. It seems likely that the oversight at Mihama-3 was a generic problem with Mitsubishi's maintenance program. However, in the case of KEPCO, the problem was exacerbated by the fact that they changed the maintenance contract for all their nuclear power plants to their subsidiary, Nihon Arm Co Ltd, in 1996. (Other power companies continued with Mistsubishi.) By changing contractors they managed to achieve a considerable reduction in the contract price and in the outage time for periodic inspections, but subsequent developments suggest that the quality of service suffered.
Belatedly, Mitsubishi noticed that pipe wall thinning was proceeding more rapidly than expected in some locations and it warned Nihon Arm of this in 1999. Nihon Arm had already noticed in 1998 that the location in question had been left off the list at Takahama-4 and it picked this up at Mihama-1 in 2002, but it didn't notice at Mihama-3 until April 2003 and didn't alert KEPCO until November of that year. KEPCO evidently didn't see this as a priority, since it decided to keep the reactor running until the next periodic inspection. Unfortunately the pipe didn't quite make it.
A further irony is that in July of this year serious wall-thinning was found in pipes at another KEPCO reactor. Main feedwater pipes in the secondary coolant system of the Ohi-1 reactor had thinned to less than the regulatory limit. A report was provided to the regulatory body, the Nuclear and Industrial Safety Agency (NISA), which duly accepted KEPCO's explanation and gave it their rubber stamp. The location in question at Ohi-1 was actually not amongst those specified in the 1990 guidelines. This is just one of several pieces of evidence that the guidelines are inadequate. Nevertheless, the discovery at Ohi-1 should have been seen as a warning.
Lessons
If this is the history, what are the lessons that can be learnt from it? The first lesson is that NISA and the Japanese power companies don't learn lessons, certainly not ones that are likely to cost them money. Profits are consistently given greater priority than safety. One would expect this tendency to be even more pronounced in a competitive electricity market. This isn't to say, of course, that an absence of competition is preferable. Rather, it indicates how out of place nuclear energy is in a people-friendly, environmentally-friendly economy.
Most other lessons also ultimately impinge on cost. For example, inspections are based on the principle that 'sampling' (i.e. testing a representative sample of the total plant) can ensure safety. It would be prohibitively expensive to regularly inspect the total length of the piping (a few thousand kilometers). However, follow-up investigations from this case have revealed that (a) the rate of thinning is different in identical pipes in different reactors and in different sections of the same reactor, and (b) the rate of thinning is not consistent over time. Under these conditions the only 'safe' solution would be to inspect them all, but power companies and regulators balk at this suggestion. Indeed there is probably some truth in their argument that inspecting everything leads to a reduction in the quality of the inspections.
There are also many lessons to be drawn about institutional failure. The refusal to respond to warnings would seem to be an instance of such a failure with both specific and less readily definable causes. It has emerged that KEPCO draws up its inspection program at least six months in advance and is unwilling to alter it, even when new information comes to light. One reason is that obtaining new parts takes time. Obviously they don't want long and costly outages while they wait for new parts to arrive. This is a very specific and understandable, albeit unforgivable, failing. But few doubt that there are more amorphous cultural failings at work as well. There are no doubt national cultural issues involved, but presumably more significant is the culture of the 'nuclear club' and of the companies themselves, KEPCO, Nihon Arm and Mitsubishi (compare Mitsubishi Motors). We should be wary, however, of concluding that simply choosing better companies will solve the problem.
Some failures which could be thought of as institutional are perhaps better described as systemic failures, because they apply across the whole nuclear industry. One such example is the Japanese nuclear industry's subcontractor system. In the Mihama-3 case, around 400 subcontractors, sub-subcontractors, etc. were to be involved in the periodic inspection that was due to begin on August 14th. The employer of the injured workers, Kiuchi Instruments, was a sub-subcontractor. But there is nothing unique about KEPCO in this regard. Workers from sub(sub...)contractors to nuclear power companies are exposed to the dirtiest and most dangerous work. It is they who receive the highest radiation doses (97% of the Japanese nuclear industry's total dose), while the power companies do everything they can to avoid liability for damages incurred (see NIT 98 article re workers' compensation case). Clearly this system is a major problem. The question of how to address it is too big to deal with here, but suffice to say that simply shifting to a system where power companies do everything in-house is unlikely to solve all the safety, communication, and other problems associated with the subcontractor system.
The final failure that I will address is the area of regulatory failure. Again this can be considered as both an institutional and a systemic failure. The principal regulatory body, NISA, rubber-stamped KEPCO's report on pipe wall thinning at Ohi-1. Its parent, the Ministry of Economy Trade and Industry (METI), when it was still MITI, before NISA was created, concurred with the industry view that the problems discovered at Surry and Trojan couldn't arise in Japan. One might ask what the regulators are there for if all they ever do is endorse the industry view. I would argue that their real function is to provide an illusion of oversight to reassure the public, in order that the nuclear industry can continue to exist. That may seem cynical, but after this case, and considering the many other failures that have come to light in the recent past, the evidence justifying that conclusion is there for all to see. The onus is on NISA and METI to prove that this conclusion is wrong, rather than on us to prove that we are right. I will go further. I will be so bold as to suggest that NISA has neither the skills nor the resources to adequately regulate and monitor the nuclear industry. If someone were to ask it now to conduct a thorough review in order to guarantee safety in the nuclear industry, it would be unable to do it.
Recommendations
There is still much that we don't know about the Mihama-3 accident. KEPCO refuses to publicly answer questions on the grounds that it is under criminal investigation. In this regard, we note that so far the only clear statement to the effect that charges will be laid relates to a breach of worker health and safety legislation. Penalties that may be incurred under this legislation are trifling. KEPCO should be tried for matters carrying heavier penalties, including professional negligence resulting in death and injury. This was a serious accident that resulted in death and injury to workers. It had the potential to lead to catastrophic damage and it was a result of serious (we believe criminal) negligence. The penalty should be accordingly severe.
Some other recommendations that logically flow from the above discussion include the following:
- In all reactors, inspect all pipes where serious wall-thinning could conceivably have occurred, not limiting the inspection to locations covered by the 1990 guidelines;
- Shut down reactors before sending workers in to make preparations for periodic inspections;
- Abandon the 'allowable defects standard', which came into effect last year in order to keep reactors operating, despite the fact that cracks have been discovered;
- Close down all old reactors.
But even if all these things were done, as long as the power companies prioritize profits over safety (which they always will do, because that's what keeps them in business) and as long as regulators are more committed to ensuring the future of nuclear energy than to ensuring safety (which they always will be, because they know that nuclear energy would become prohibitively expensive and technologically impossible if they really tried to make it safe) it still wouldn't be enough. So we are left, as usual, calling for an end to nuclear energy. In doing so, we find grounds for hope in the fact that the public's distrust of nuclear energy continues to grow, and we pray that people won't get panicked into choosing nuclear energy as a solution to global warming.
(1) The secondary system is associated with the turbine, as opposed to the primary system, which is associated with the reactor itself.
(2) The pipe which ruptured was made of carbon steel. Its external diameter was 560mm and it was located between the fourth low-pressure feedwater heater and the de-aerator, on the second floor of the turbine building.
(3) Altogether, there are three steam generators (A, B and C).
(4) Boron acts as a neutron absorber. By absorbing surplus neutrons it helps to prevent the reactor from going critical again.
(5) In fact, Japan is the only country to append '+' and '-' signs to its INES ratings. It only does this in the case of '0' ratings. INES ratings are determined by the country in which the accident occurs.
Philip White
International Liaison Officer and Editor of Nuke Info Tokyo
Click here for other reports about the Mihama-3 accident
Return to NIT 102 contents


{kind=link}