Updates on the 311 Children’s Thyroid Cancer Trial
Ido Ken’ichi, Attorney
1. Introduction
I wrote about the filing of the 311 Children’s Thyroid Cancer Suit in the March/April 2022 issue of Nuke Info Tokyo. cnic.jp/english/?p=5973 In this report I introduce how the trial has developed since then.
The plaintiffs of the suit were initially six people (two men and four women) aged 17 to 27 years at the time of the filing (6 to 16 at the time of the Fukushima nuclear accident). A woman who was 12 years old at the time of the accident joined the group later, bringing the number of plaintiffs to seven. Oral proceedings have already been held eight times. The gallery seating area in the Tokyo District Court is limited, but about 200 people gathered each time, which was very encouraging for the plaintiffs.
2. Plaintiffs’ testimonies
Each plaintiff delivered testimony in court, presenting their thoughts to the judges. Due to space restrictions here, I introduce the testimonies of three plaintiffs.
Plaintiff A was found to have thyroid cancer as a high-school student. After having a lobectomy, the plaintiff entered university, but later had a recurrence of the cancer, losing the entire thyroid gland. The plaintiff had little option but to discontinue university studies and gave up the dream of a lifetime. “Friends who live their lives as they like to make me envious, and such envy makes me depressed,” the plaintiff said. “The cancer has metastasized to the lung, and I hope the disease will not get worse.” Plaintiff B, who was discovered to have thyroid cancer as a middle-school student, underwent removal surgery twice, losing the entire thyroid gland. The plaintiff says: “Everything changed before I established my own way of thinking, my character, and my future dream. I don’t know what I want to do in the future. I would like to be economically stable. I have given up on love, marriage, and childbirth.” Plaintiff C, discovered as having thyroid cancer as a high-school student, also had surgery twice and lost the entire thyroid gland. “I have a vague sense of anxiety and cannot think about the future,” said the plaintiff in delivering testimony. “However, it is good that it is me who got the disease, because it would have been harder if a friend or relative had gotten it.”
The conditions surrounding the plaintiffs are varied and some of them suffer poor health. However, I feel that the young plaintiffs are growing up steadily, thanks mainly to the courage given by many people’s support, the confidence gained from the fact that they completed their court testimonies, and deepened mutual trust among themselves.
3. Arguments in the trial
The greatest point of dispute in this trial is the causal relationship between radioactive exposure resulting from the Fukushima nuclear accident and the thyroid cancer of the plaintiffs. Concerning this point, the plaintiffs and defendant argue as follows:
(1) Plaintiffs’ argument
The main point of the argument is that children in Fukushima, including the plaintiffs, had their thyroid exposed to radiation to some degree. As a result, the Fukushima Prefectural Health Survey found many pediatric thyroid cancer cases. We requested Dr. Tsuda Toshihide, Professor at Okayama University, to calculate the probability that the plaintiffs’ thyroid cancer was caused by the radioactive exposure (“causation probability”), concluding that the probability was 95% to 99%. Accordingly, the relationship between the radioactive exposure and plaintiffs’ thyroid cancer should be legally confirmed.
(2) TEPCO’s argument
TEPCO’s counterargument can be summarized as follows:
i) Thyroid cancer does not develop unless the thyroid dose is in excess of 100 mSv (“100 mSv threshold argument”).
ii) The plaintiffs’ thyroid doses due to the Fukushima accident are at most 10 mSv.
iii) Therefore, the cause of the plaintiffs’ thyroid cancer is not exposure to radiation. The many pediatric thyroid cancer cases found by the Prefectural Health Survey are “latent cancer” (which does not produce symptoms even if left untreated). A proportion of those children had latent thyroid cancer from before.
(3) Plaintiffs’ argument against the TEPCO argument
The plaintiffs argue against TEPCO as follows:
i) 100 mSv threshold hypothesis
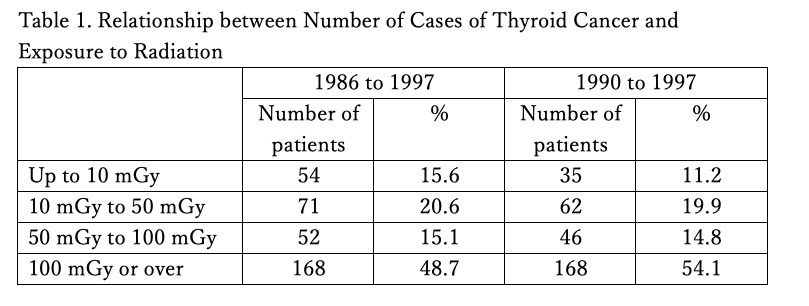
There is no data that backs up the hypothesis that thyroid cancer does not develop unless the thyroid dose exceeds 100 mSv. The thyroid doses of the children who contracted pediatric thyroid cancer in Ukraine after the Chernobyl nuclear disaster are shown in the table below. According to the table, the doses of about half the children were less than 100 mSv. It is known that thyroid cancer developed even if the thyroid dose was 50 mSv, 30 mSv, or 10 mSv[1] (1 mGy in this table is deemed to be 1 mSv).
ii) Thyroid doses
Thyroid doses are dependent largely on the internal exposure due to radioactive iodine taken into the body. To learn precisely how much the thyroid of a child was exposed to radiation, it is necessary to directly measure thyroid radiation immediately after exposure. Iodine I-131 taken into the thyroid, decays at a physical half-life of eight days, and the dose becomes unmeasurable over time. Following the Chernobyl nuclear disaster, the then Soviet Union directly measured the radiation of the thyroids of hundreds of thousands of children. On the other hand, Japan discontinued direct thyroid radiation measurement after measuring 1,080 children in Iitate Village, Kawamata Town, and Iwaki City. As a matter of course, the plaintiffs did not undergo direct thyroid measurement.
Because of the lack of directly measured data, the thyroid doses of children in Fukushima can only be known by an estimation of internal exposure to radioactive iodine. The routes of internal exposure include inhalation intake (respiratory intake of radioactive iodine in the atmosphere into the body) and oral intake (intake of radioactive iodine in food and drinking water into the body). The inhalation intake can be calculated if time-based radioactive iodine concentration data in the atmosphere is available, whereas accurately estimating the oral intake is extremely difficult, because it needs to be calculated based typically on the types of water taken into the body (tap water, well water, etc.), the varieties and locations of production of produce taken in, how the produce was cultivated (open-field farming or greenhouse farming), when the produce was cultivated, and the estimated contamination concentration of each food product.
The basis on which the defendant asserts that the plaintiffs’ thyroid doses were no more than 10 mSv comes from the UNSCEAR (United Nations Scientific Committee on the Effects of Atomic Radiation) 2020/2021 Report. UNSCEAR, in its 2013 Report, tentatively estimated that a 10-year-old in Fukushima Prefecture (except children in the evacuation zones) received a dose of 15 mSv to 31 mSv of radiation to the thyroid, but in its 2020/2021 Report, the estimation was significantly reduced to 1 mSv to 17 mSv.
The estimation method used by UNSCEAR includes many problems in both terms of inhalation intake and oral intake. Here, I will indicate a serious problem concerning UNSCEAR’s estimation of inhalation intake.
Concerning inhalation intake, UNSCEAR stated that no monitoring data that would show time-based changes in the radioactive iodine concentrations in the atmosphere was available, and employed the estimations obtained by the Atmospheric Transport Diffusion and Deposition Model (ATDM) method, in which changes over time of the types and volumes of radioactive substances in the atmospheric air at specific locations are estimated based on the “source terms” (changes in the types and volumes of radioactive substances discharged from the reactor building to the environment), land features, and meteorological conditions, and determined that a 10-year-old who lived in Fukushima City inhaled an average of 5.1 mGy (or 5.1 mSv in sieverts) during the one year period after the accident.
However, this estimation is based on hypotheses combined with assumptions, and its accuracy is very doubtful. As an example, chronological atmospheric radioactive iodine concentrations could have been calculated based on the data of a monitoring post in the Momijiyama Park located near the center of Fukushima City, but UNSCEAR deliberately ignored the data. With this data, we requested Dr. Kurokawa Shin’ichi, Professor Emeritus of the High Energy Accelerator Research Organization, to calculate the thyroid inhalation intake of children in Fukushima City. The conclusion was that a one-year-old in the city would have had a thyroid dose of about 60 mSv just through respiration alone under the plumes that hit the city on March 15 and 16, 2011. This conclusion made it clear that the UNSCEAR estimation and the argument of the defendant, Tokyo Electric Power Company Holdings Inc. (TEPCO), are baseless.
iii) The latent cancer hypothesis
The argument that denies the relationship between many pediatric thyroid cancer cases discovered by the Prefectural Health Survey and radioactive exposure is at times called the “screening effect” or “overdiagnosis hypothesis.” TEPCO argues that those cancer cases are latent. It is necessary to spell out these hypotheses.
If a mass inspection (screening) is conducted irrespective of whether a person has thyroid cancer symptoms or not, as the Fukushima Prefectural Health Survey was, latent stage cancer may be discovered. Even if screening were not conducted, such latent cancer would grow gradually and eventually manifest itself as a kind of symptom. In this case, the screening discovered cancer before its manifestation. This can be called the “screening effect in the narrow sense.”
TEPCO’s latent cancer argument is different. The operator argues that the pediatric thyroid cancer cases discovered by the Fukushima Prefectural Health Survey are latent and that even if they were left untreated, they would not manifest clinical symptoms (the cancer would remain latent for a lifetime), so lobectomy would not be required.
The basis on which TEPCO insists on the latent cancer argument is that a given rate of dissected human bodies is found to have thyroid cancer the individuals were unaware of (because it was latent) when they were alive. The operator also argues that, in South Korea, a rapidly increasing number of thyroid cancer cases were found after mass thyroid checks became common; however, even though such cancers were removed, there was no change in the number of deaths due to thyroid cancer (implying that lobectomy was not required).
The plaintiffs do not deny the possibility of the screening effect in the narrow sense. However, as noted in the previous report, the screening effect does not explain why the number of pediatric thyroid cancer cases in Fukushima increased several ten of times.
The plaintiffs also agree that a great portion of adults (especially the aged) have latent cancer. However, no available data indicates that children have latent cancer. Even though there may be a given proportion of latent pediatric cancer cases, it does not explain such an outbreak.
In addition, the Fukushima Prefectural Health Survey program is designed carefully to prevent unnecessary thyroid lobectomy, namely, not to remove latent cancers, as explained below:
1) Even when ultrasound testing finds a nodule of 5 mm or less, it is not subjected to secondary testing (even though such a nodule can be cancerous). Most latent cancers are tiny, 5 mm or less.
2) A nodule of 5.1 mm or more is subjected to secondary testing. However, whether fine needle aspiration biopsy should be conducted or not to determine whether the nodule is cancerous or not is carefully examined. All the cases having a nodule of 20.1 mm or more undergo fine needle aspiration biopsy. When a nodule is between 10.1 mm and 20.0 mm, the patient undergoes biopsy when at least one test item of the total of seven items indicates malignancy. When the nodule is between 5.1 mm and 10.0mm, the case proceeds to biopsy when all the seven test items indicate malignancy.
3) When the results of a biopsy indicate malignancy, it does not mean that the patient immediately undergoes lobectomy. The degree of disease advancement, whether an extracapsular spread exists or not, whether lymph node metastasis and/or distant metastasis exists, and the size, position, and other characteristics of the tumor, are carefully examined. Lobectomy is conducted when it is found applicable to the case according to the guidelines.
The cases that have undergone thyroid lobectomy after such prudent examination are extremely unlikely to have been latent.
In addition, Dr. Suzuki Shin’ichi, who operated on most pediatric thyroid lobectomy cases at Fukushima Medical University, reports as follows:
“Up until December 31, 2018, the Fukushima Medical University Thyroid and Endocrine Surgery Division performed 180 thyroid cancer surgeries. The average age at the time of diagnosis and that at the time of the accident were, respectively, 17.9 years and 13.3 years. The average size of the tumors was 16 mm. Of the cases, 175 had papillary cancer; 72% showed lymph node metastasis; 47% showed spread to the tissue/organ adjacent to the thyroid; and 1.7% showed lung metastasis.”
The cases where lobectomy was conducted after being found applicable were not mild. They were not latent cancer cases, which would not require surgery. Dr. Suzuki is clear that there was no room for overdiagnosis.
The above is a summary of the arguments delivered so far in court. The dispute will continue in court, and we plan to add the argument that the cases of the plaintiffs were never latent, based on their specific cases. TEPCO asserts that the many pediatric thyroid cancer cases discovered by the Fukushima Prefectural Health Survey were latent, but does not answer the question of whether the plaintiffs had latent cancer or not.
4. Future challenges
As stated in the previous report, pediatric thyroid cancer is a very rare disease. Normally, one or two cases are found in every one million persons per year. According to the release of the Fukushima Prefectural Health Survey Review Committee of November 24, 2023, at least 363 people were diagnosed with pediatric thyroid cancer and 261 of them have undergone surgery[2], among about 380,000 who were 18 years old or younger at the time of the nuclear accident. Compared with the days before the Fukushima nuclear accident, this is clearly an outbreak involving an increase of several tens of times. This outbreak cannot be explained by the screening effect in the narrow sense or by the latent cancer hypothesis. In court, plaintiffs’ arguments are far stronger than TEPCO’s. The issue is whether the court can deny the arguments of UNSCEAR, the national government, and Fukushima Prefecture, all of which back up the operator. To encourage the court to do so, the understanding that the outbreak of pediatric thyroid cancer in Fukushima is attributable to nuclear exposure needs to be more widely and deeply known among citizens.
5. Conclusion
The most striking characteristic of this case is that plaintiffs cannot come out publically (cannot publicize their names and faces). The plaintiffs, who hold no responsibility for the nuclear power accident, were forced to be cancer survivors at young ages and filed this suit to question the responsibility of the perpetrator. However, they need to be anonymous and faceless because otherwise they would be subject to severe criticism and discrimination from society. They cannot present their arguments to society with their faces open to view. I would like this problem of Japanese society to be understood.
To change this situation, we firstly need to try to have the trial known and the plaintiffs’ voices heard by as many people as possible. The mainstream media does not report on this lawsuit. As such, small-scale media and oral communication are important. In this sense, I am very thankful to have this opportunity of contributing this article to CNIC. I would like the readership to take an interest in and support this case. We have a website “311 Thyroid Cancer Children Support Network” and I would appreciate it very much if you would visit us there (www.311support.net/).
Please also see the following links to English translations of testimonies from plaintiffs:
“I started prioritizing treatment over my dreams for the future”: Public testimony of a young woman diagnosed with thyroid cancer after Fukushima disaster
[1] Mykola Tronko, Ph.D., et al. “Thyroid carcinoma in children and adolescents in Ukraine after the Chernobyl nuclear accident.” Cancer. 1999 Jul 1;86(1):149-56.
[2] OurPlanet-TV website at www.ourplanet-tv.org/47901/